| Case report | Peer reviewed |
Cite as: Hough SD, Jennings SH, Almond GW. Thiamine-responsive neurological disorder of swine. J Swine Health Prod. 2015;23(3):143–151.
Also available as a PDF.
SummaryThis report describes a thiamine-responsive neurological disease and the methodology leading to its diagnosis. The initial case involved one nursery farm. Approximately 5% of pigs at 5 to 7 days after weaning exhibited central nervous system signs. Over the next 3 weeks, 16 of the company’s 41 nursery farms had pigs with similar clinical signs. One month later, neurologic signs were observed in unweaned piglets in several sow farms. Pigs were weaned at approximately 19 days and moved to off-site nurseries. Live pigs and fresh and formalin-fixed samples from acutely affected pigs were sent to diagnostic laboratories. Feed samples were submitted for mycotoxin and nutrient analyses. Initial reports revealed no precise cause of the neurological condition; however, polioencephalomalacia (PEM) subsequently was identified in affected pigs. A field trial determined the response to treatment with atropine, a vitamin A, D, and E preparation, or vitamin B12 plus thiamine. Pigs treated with thiamine recovered from the neurological condition. Upon implementation of thiamine injections on a company-wide basis, neurological signs associated with PEM were no longer evident. The authors do not recommend routine thiamine injections under normal circumstances. In this case, compromised dietary thiamine levels during feed manufacturing possibly contributed to the PEM. | ResumenEste reporte describe la enfermedad neurológica con respuesta a la tiamina y la metodología que llevó a su diagnóstico. El caso inicial involucró un sistema de destete. Aproximadamente 5% de los cerdos de 5 a 7 semanas después del destete exhibieron signos relacionados con el sistema nervioso central. Durante las siguientes 3 semanas, 16 de las 41 granjas de destete de la compañía tuvieron cerdos con signos clínicos similares. Un mes después, se observaron signos neurológicos en lechones no destetados en varias granjas de pie de cría. Los cerdos se destetan a los 19 días aproximadamente y son trasladados a destetes fuera de sitio. Se enviaron al laboratorio de diagnóstico cerdos vivos y muestras frescas y fijadas en formalina de cerdos afectados de forma aguda. Se enviaron muestras de alimento para análisis de micotoxinas y nutrientes. Los reportes iniciales no revelaron una causa precisa de la enfermedad neurológica; sin embargo, subsecuentemente se identificó polioencefalomalacia (PEM por sus siglas en inglés) en los cerdos afectados. Una prueba de campo determinó la respuesta al tratamiento con atropina, una preparación de vitamina A, D, y E, o vitamina B12 más tiamina. Los cerdos tratados con tiamina se recuperaron de la enfermedad neurológica. Después de la implementación de la inyección de tiamina en todos los cerdos de la compañía, los signos neurológicos asociados con el PEM ya no se manifestaron. Bajo circunstancias normales, los autores no recomiendan las inyecciones rutinarias de tiamina. En este caso, los niveles de tiamina en la dieta, afectadas durante la preparación del alimento, posiblemente contribuyeron al PEM. | ResuméLe présent rapport décrit une maladie neurologique répondant à la thiamine et la méthodologie menant à son diagnostic. Le cas initial impliquait une pouponnière. Cinq à 7 jours suivant le sevrage environ 5% des porcs démontraient des signes d’atteinte du système nerveux central. Durant les 3 semaines qui suivirent, dans 16 des 41 pouponnières que possèdent l’entreprise des porcs ont présenté des signes cliniques similaires. Un mois plus tard, des signes neurologiques furent observés chez des porcelets non-sevrés dans plusieurs des fermes de maternité. Les porcs furent sevrés à environ 19 jours et déménagés à une pouponnière hors-site. Des porcs vivants et des échantillons de tissus frais et fixés dans la formaline provenant de porcs affectés de manière aiguë furent acheminés à des laboratoires de diagnostic. Des échantillons de nourriture furent soumis pour analyse des nutriments et détection de mycotoxine. Les rapports initiaux ne démontraient aucune cause précise de la condition neurologique; toutefois, une polioencéphalomalacie (PEM) subséquente fut identifiée chez les porcs atteints. Un essai clinique a déterminé la réponse à un traitement avec de l’atropine, une préparation de vitamines A, D, et E, ou de la vitamine B12 plus thiamine. Les porcs traités avec de la thiamine ont récupéré de la condition neurologique. Avec la mise-en-place d’injections de thiamine à l’ensemble des animaux de la compagnie, les signes neurologiques associés à la PEM n’étaient plus évidents. Les auteurs ne recommandent pas l’injection de thiamine sur une base routinière dans des circonstances normales. Dans le cas présent, des niveaux de thiamine alimentaire déficients durant la préparation de l’aliment ont possiblement contribué à la PEM. |
Keywords: swine, polioencephalomalacia, thiamine, neurological signs
Search the AASV web site
for pages with similar keywords.
Received: May 30, 2014
Accepted: December 11, 2014
Polioencephalomalacia (PEM) is recognized as an important neurologic disease of ruminants. In contrast to PEM in ruminants, thiamine (vitamin B1) deficiencies, and specifically neurologic signs associated with thiamine deficiencies, are rarely reported for swine.1 Anorexia, reduced weight gain, occasional vomiting, and sudden death are considered the common clinical signs associated with thiamine deficiency in pigs.2 In addition, thiamine supplementation of modern pig diets provides limited benefit, as primary feed ingredients contain sufficient thiamine to meet the requirements of pigs.3,4
Thiamine depletion requires considerable time in pigs, and it may take up to 35 days for pigs to exhibit non-neurologic clinical signs.5,6 Dietary deficiency of thiamine apparently is rare, with a few notable case reports;7,8 however, excessive sulfur intake as a result of diet manipulation was noted as a potential cause of thiamine deficiency.6 The precise number of cases of thiamine deficiency in the modern pork industry is unknown.
When it comes to the clinical presentation of disease outbreaks, nutritional deficiencies and alterations to the diet are often low on the list of differential diagnoses. This report describes a thiamine-responsive neurological disease and the diagnostic methodology that led to its discovery.
Clinical description
The chronological events are important to comprehend the changes and extent of this particular case. Thus, the clinical description reviews the events as the clinical signs evolved in several different farms in a production system with over 100,000 sows. All farms were PQA Plus certified, following the guidelines provided by the National Pork Board, prior to the clinical problems.
In February 2012, approximately 5% of the pigs in one of the company’s nursery farms exhibited central nervous system signs, with onset of clinical signs 5 to 7 days after weaning at approximately 19 days of age. Clinical signs included ataxia and standing with front legs splayed and head extended, stargazing, trembling, and hyperesthesia (Figure 1). Some pigs entered into lateral recumbency and were unable to rise. Pigs were identified as affected by stimulating them to move about the pens. The affected pigs ran into feeders, cup drinkers, penning material, and other pigs, suggesting another undefined problem. These pigs proceeded to exhibit other previously described neurologic signs for PEM. Mortality of affected pigs was 100%. No consistent gross lesions were identified on necropsy of five pigs.
Figure 1: Neurologic signs, such as ataxia, splayed front legs, stargazing, trembling and hyperesthesia, were observed in pigs 5 to 7 days after weaning in one nursery farm. Within 3 weeks, similar neurologic signs were noted in pigs at several nursery farms. This figure illustrates the neurologic posture in a nursery pig exhibiting typical clinical signs of the case.

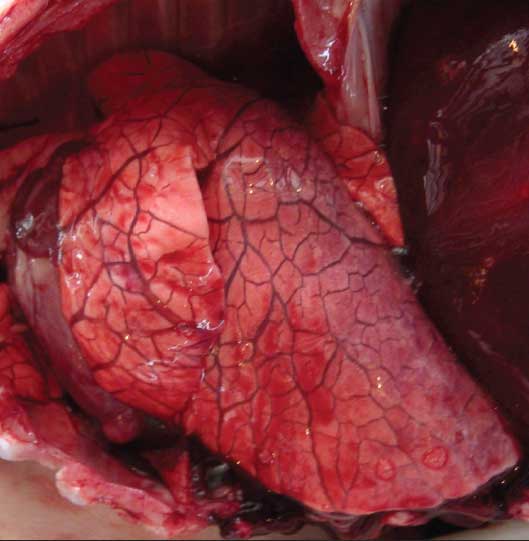
Concurrent to the clinical signs in the nursery, a separate flow of feeder pigs was placed into a finisher barn. The feeder pigs were from a different nursery and were company owned. Their feed was processed in the same feed mill as the feed for the nursery pigs. At placement, 43 animals (approximately 10%) had died on the truck during transport and an additional 25 pigs (approximately 6%) became dyspneic, vocalized, and began to die within 2 hours of being placed into pens. The pens were not crowded and the ambient temperature was 11°C. Necropsy of 20 pigs revealed severe pulmonary edema and copious amounts of serous pleural fluid (Figure 2). Most pigs also had moderate liver congestion, and three pigs had cranioventral pneumonia and mildly edematous mesentery. Samples submitted to the Iowa State Veterinary Diagnostic Laboratory included fresh and formalin-fixed samples of lung, heart, lymph node, liver, spleen, kidney, intestine, brain, and tonsil, as well as serum from affected and unaffected animals.
Figure 2: Severe pulmonary edema in a feeder pig. In addition to the neurologic signs observed in pigs at several nursery farms (Figure 1), pulmonary edema was a common finding in several pigs.
Over the next 3 weeks, the prevalence of the neurologic signs in nursery pigs increased to involve 16 of the 41 nurseries in the company’s North Carolina system. Signs also were observed in weaned pigs from North Carolina that were sent to company-owned, wean-to-finish facilities in Iowa. One month after the index case, the same clinical signs were seen in a North Carolina sow farm in 23-day-old pigs, 2 days before weaning. Within the subsequent week, the neurologic signs in more sow farms began to be observed in pigs just prior to weaning. The incidence of neonatal diarrhea also increased in numerous sow farms across the system.
Two nurseries that had not experienced the neurologic signs in young pigs began to have a sudden increase in mortality in pigs 2 to 3 weeks after placement. As in the index feeder-pig case, these pigs showed few clinical signs other than dyspnea before dying. Also, some pigs appeared to be vomiting. Necropsy revealed severe pulmonary edema and copious amounts of serous pleural effusions. Injections of isoflupredone acetate, ceftiofur, enrofloxacin, and florfenicol, as well as various water medication strategies (soluble penicillin, chlortetracycline, and tiamulin) did not prevent clinical signs or reduce their severity.
Losses
A marked increase in weekly nursery mortality (Figure 3) occurred during late March and April, representing the loss of approximately 12,000 pigs in the production system during the period, compared to normal mortality levels.
Figure 3: Neurologic signs were observed in pigs 5 to 7 days after weaning in several nursery farms in North Carolina. As a result of the neurologic condition, mortality increased in the nursery farms of the company. This figure depicts weekly nursery mortality for 38 weeks (January through September 2012).
Initial diagnostic tests
A differential list of causes for the neurologic syndrome included Streptococcus suis, Haemophilus parasuis, water deprivation, edema disease due to enterotoxigenic Escherichia coli, organophosphate toxicosis, nutritional imbalance, and porcine enterovirus and hemagglutinating encephalomyelitis virus. A differential list of causes for fatal pulmonary edema included fumonisin toxicosis, porcine circovirus, influenza, and porcine reproductive and respiratory syndrome (PRRS) virus.
Fresh and formalin-fixed samples from acutely affected pigs were sent to diagnostic laboratories, while samples of the feed were submitted for the isolation, enumeration, and identification of any species of molds detected (JKM Lab, Mount Prospect, Illinois), toxin testing (vomitoxin, aflatoxin, zearalenone, fumonison, 15 trichotheces) at North Dakota State University Veterinary Diagnostic Laboratory (Fargo, North Dakota), organophosphate testing at Diversified Laboratories (Chantilly, Virginia), and heavy-metal screening (arsenic, cadmium, cobalt, chromium, lead, mercury) at Carolina Analytical Services (Bear Creek, North Carolina). Feed samples were also tested at the feed-mill laboratory for fumonisins, deoxynivalenol, and zearalenone. Live pigs displaying clinical signs (n = 29) also were submitted to various diagnostic laboratories.
Feed evaluation
All nursery feed was pelleted. On the premise that the neurologic signs were strikingly similar to PEM in cattle and the preliminary findings that injections of thiamine elicited positive responses, feed samples were evaluated for thiamine concentrations. Diagnostic evaluation of the complete feed revealed a thiamine level of 0.62 mg per kg, which represents only 18% of the expected 3.5 mg per kg. Mycotoxin evaluation showed that all feed samples were negative for aflatoxin, fumonisins, and deoxynivalenol. Samples were negative for tremorgens, pesticides, and heavy metals.
Initial postmortem findings
Fourteen nursery-pig submissions (one to five pigs per submission) initially were submitted to diagnostic laboratories. Brain lesions were not identified in the initial pig submissions (Table 1). Subsequent submissions included pigs with meningeal thickening and neutrophilic inflammation of the brain, as well as cortical necrosis and edema suggestive of S suis or H parasuis. There was growth of S suis from a brain swab of an individual pig, but other swabs and tissues did not yield bacterial growth. The ninth nursery-pig submission revealed lesions of PEM of the cerebral cortex, and the lesion was seen in the remaining six nursery pigs submitted. Heavy metal testing was unremarkable in all cases.
Table 1: Diagnostic results obtained from submissions of one or more pigs to diagnostic laboratories*
| Date | Farm | Pig age (weeks) | Brain lesions | Other lesions |
|---|---|---|---|---|
| 22 Feb | Index NC case, Nursery 1 | 4 | None | Atrophic enteritis, multifocal dilation of colonic crypts |
| 22 Feb | Index NC case, Finisher 1 | 10 | None | Pulmonary edema, cardiac congestion, hepatic congestion |
| 22 Feb | Nursery 2 | 4 | None | Villous atrophy, ileum |
| 29 Feb | Nursery 3 | 3 | Brain hemorrhage | Epicarditis, interstitial pneumonia |
| 29 Feb | Nursery 4 | 4 | None | Focal myocardial hemorrhage, interstitial pneumonia |
| 7 Mar | Nursery 5 | 4 | Meningeal thickening and neutrophilic inflammation | Villous atrophy of ileum; broncho- and interstitial pneumonia |
| 9 Mar | Nursery 6 | 3 | Purulent meningitis | Interstitial pneumonia, glomerulonephritis |
| 21 Mar | Index NC case, Sow Farm 1 | 3 | Focal neovascularization in cerebral cortex | Lymphocytic gastritis, villous atrophy, jejunum |
| 23 Mar | Sow Farm 2 | 3 | None | Nephritis |
| 23 Mar | Nursery 7 | 4 | Cortical necrosis with edema | Necrotizing bronchiolitis, fibrinous pleuritis; thickened colonic mucosa |
| 27 Mar | Index IA case, Wean-to-finish 1 | 3 | Meningeal edema, perivascular hemorrhage, rare neutrophils | Villus blunting, small intestine |
| 27 Mar | Wean-to-finish 2 | 3 | None | Bronchopneumonia |
| 27 Mar | Nursery 8 | 4 | Focal areas of malacia, gliosis, and necrosis | Atrophic enteritis |
| 27 Mar | Nursery 7, 2nd set of samples | 3 | Perivascular lymphocytic cuffing and subdural congestion | None |
| 28 Mar | Nursery 9 | 4 | Polioencephalomalacia, cerebral cortex; leukoencephalomalacia | Villous atrophy, jejunum |
| 28 Mar | Sow Farm 1, 2nd set of samples | 3 | Non-suppurative meningitis | None |
| 28 Mar | Nursery 10 | 4 | Multifocal polioencephalomalacia, cerebral cortex, and nucleus of brainstem | None |
| 28 Mar | Nursery 11 | 4 | Multifocal polioencephalomalacia, cerebral cortex | None |
| 30 Mar | Sow Farm 3 | 3 | None | None |
| 30 Mar | Nursery 12 | 6 | None | Pulmonary edema; diffuse hepatic vacuolization |
| 4 Apr | Wean-to-finish 3 | 3 | Neuronal necrosis and polioencephalomalacia, cerebral cortex | Atrophic enteritis, interstitial pneumonia |
| 4 Apr | Nursery 13 | 6 | None | Pulmonary edema, suppurative bronchointerstitial pneumonia, necrotizing bronchiolitis |
| 18 Mar | Nursery 14 | 4 | Mononuclear cells, meninges of the brain | Interstitial pneumonia, glomerulonephritis |
* Neurologic signs were observed 5 to 7 days after pigs were weaned at approximately 19 days of age in several nursery farms in North Carolina. The table does not include findings from the College of Veterinary Medicine, North Carolina State University.
Severe pulmonary edema was observed in one finishing-pig submission. Microscopic lesions confirmed pulmonary edema as well as extensive congestion of cardiac and hepatic tissue. Evaluation of serum yielded hypovitaminosis D and increased alkaline phosphatase. No etiologic agent was suggested. Among three wean-to-finish submissions were two revealing meningeal edema and bronchopneumonia. Pigs were diagnosed with PRRS and hypovitaminosis A and D. Lesions of PEM and neuronal necrosis, as well as interstitial pneumonia, were observed in the third finishing pig submission. Brain sodium levels were tested and were considered low (1439 mg per kg) and below the threshold of 2000 mg per kg for salt toxicosis.
Among three sow-farm submissions, two piglets had focal necrosis of the cerebral cortex and non-suppurative meningitis of unknown etiology. Samples were negative for porcine enterovirus and hemagglutinating encephalomyelitis virus. In the third submission, there were no lesions, and cholinesterase activity in the brain was normal.
Summary of diagnostic findings
The diagnostic findings included 23 accessions (Table 1). Complete necropsy results were obtained from 23 pigs at laboratories other than North Carolina State University (NCSU). Of these pigs, 15 (61%) were identified as having brain lesions: six (26%) were described as having PEM or cortical necrosis of the cerebrum, three (13%) had mononuclear inflammation, three (13%) had neutrophilic or mixed inflammation, and three (13%) had other non-inflammatory brain lesions, including edema, hemorrhage, or neovascularization. One pig with PEM also had areas of mixed meningeal inflammation.
The majority of pigs submitted for diagnostic evaluation were positive for PRRS virus by PCR testing. In addition, some pigs tested positive for swine influenza virus or rotavirus.
Postmortem findings from North Carolina State University
Eight 16- to 18-day old pigs (five females, three males) ranging from 3.8 to 7.0 kg (average 5.8 kg) and showing neurological signs, were examined at NCSU immediately after euthanasia. Six of the eight pigs (75%) exhibited moderate to marked multifocal laminar cerebrocortical necrosis that fluoresced under 365-nm ultraviolet (UV) light from a Wood’s lamp. Histologically, the cerebral cortex contained multiple relatively well-demarcated zones of coagulative necrosis, most severe along the grey-white interface of the frontal lobe, but also present in the parietal lobe (Figures 4, 5, and 6). In the early stages or in mild cases, lesions were often limited to middle and deep portions of cerebrocortical sulci, with progression to involve entire gyri. Affected areas had rarefied neuropil with prominent capillaries lined by hypertrophied endothelial cells. These vessels, and vessels of the overlying meninges, were often cuffed by edema and occasionally by one to three layers of lymphocytes, plasma cells, and very rare eosinophils (Figure 7). Neurons in these areas were frequently necrotic with shrunken angular profiles, cytoplasmic eosinophilia, and loss of Nissl substance (Figures 5 and 7). Alzheimer type II cells were also frequently present individually or in pairs or clusters of up to four cells with enlarged, glassy nuclei and peripheralized chromatin (Figure 6). Vacuolation of the periventricular grey matter of the brainstem was seen in five pigs. Three of these five pigs also had infiltration of Alzheimer type II cells in these areas, with neuronal necrosis at this location in two pigs (Figures 8 and 9).
Figure 4: Neurologic signs were observed in pigs 5 to 7 days after weaning in several nursery farms in North Carolina. Within 2 months, the clinical signs were observed in pigs prior to weaning. Figures 4 to 9 provide the descriptions of histopathology associated with pigs (17 days of age) submitted to the College of Veterinary Medicine, North Carolina State University. Cerebral cortex; Pig 5. The left half of the image exhibits an extensive area of laminar, neuronal necrosis (N) and neuropil rarefaction due to edema with a relatively abrupt transition to viable cerebral cortex (V) on the right side of the image. There is a mild, mononuclear infiltrate within the overlying meninges. Hematoxylin and eosin, 4× magnification.
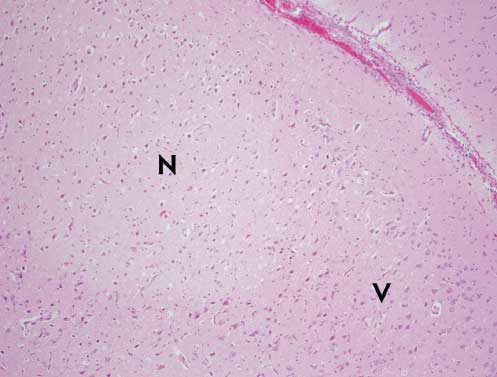
Figure 5: Cerebral cortex; Pig 5. Higher magnification of neuronal necrosis shown in Figure 4. The necrotic neurons are shrunken and angular with hypereosinophilic cytoplasm and pyknotic nuclei (arrows). Vessels in the section are lined by hypertrophied endothelial cells. Necrotic neurons and vessels are surrounded by edema. Hematoxylin and eosin, 40× magnification.
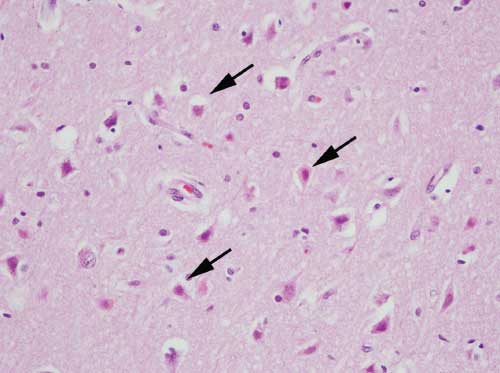
Figure 6: Cerebral cortex; Pig 5. Higher magnification of viable cortex shown in Figure 4. There is mild gliosis characterized by increased numbers of enlarged astrocytes (arrows) with vesicular nuclei that are occasionally present in pairs (Alzheimer’s type II astrocytes). Hematoxylin and eosin, 40× magnification.
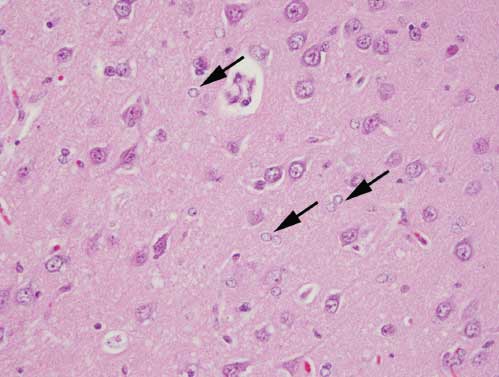
Figure 7: Cerebral cortex; Pig 8. High magnification of meningeal infiltrate overlying a region of cortical necrosis reveals small numbers of eosinophils (E) in addition to the mononuclear cells seen in most of the affected pigs. A necrotic neuron (arrow) is present in the top left of the field. Hematoxylin and eosin, 100× magnification.
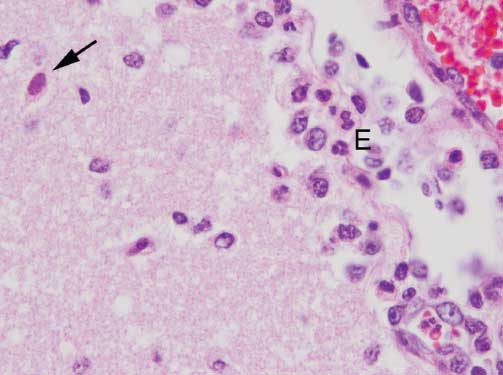
Figure 8: Brainstem; Pig 2. There is a focus of neuronal necrosis (N), neuropil vacuolation, and mild, mononuclear cell perivascular cuffing (arrow) within the periventricular grey matter. Hematoxylin and eosin, 20× magnification.
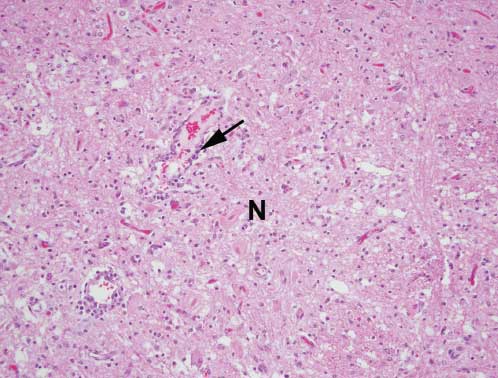
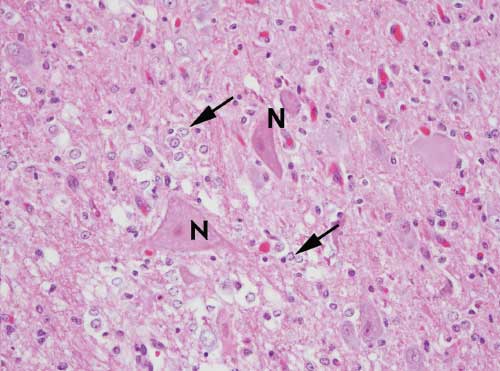
Figure 9: Brainstem; Pig 2. Higher magnification of neuronal necrosis (N) and neuropil vacuolation shown in Figure 8. Additionally, several Alzheimer’s type II astrocytes (arrows) are present. Hematoxylin and eosin, 40× magnification.
Treatment trial
While investigators waited for the final diagnostic results from NCSU, 24 pigs exhibiting clinical signs in one facility were placed in three experimental treatment groups (n = 8 pigs per group). Pigs in Group 1 were treated intramuscularly (IM) with 5 mg of atropine sulfate. Pigs in Group 2 received (IM) 1 mL of a product containing vitamin A (50,000 IU), vitamin D (50,000 IU), and vitamin E (500 IU). Pigs in Group 3 were injected IM with 1 mL (100 mg) of vitamin B12 and 1 mL (100 mg) of thiamine (vitamin B1). The following day, each pig was assessed. The pigs injected with atropine were still alive but recumbent. The pigs injected with the fat soluble vitamin mixture were also recumbent. The pigs injected with the vitamin B compounds were no longer recumbent and appeared to be eating and drinking. Subsets of pigs at two other farms were then injected with thiamine alone and similar positive results were observed. A solution of mixed B vitamins, which included 200 mg thiamine per mL, was distributed to all the nurseries and sow farms for treatment and prophylactic administration to weaning-age pigs and sows. Upon implementation of the thiamine injections, neurological signs associated with the thiamine-induced PEM were no longer evident.
Discussion
Although PEM has been reported in a variety of species, including foxes,9 mink,9 dogs,10,11 cats,11,12 and camels,13 few reports historically described thiamine-responsive PEM in pigs.8 The most commonly described condition for laminar cortical necrosis in the pig is salt toxicosis; however, due to the widespread nature of the epidemic, including several farms, and the paucity of eosinophils histologically, salt toxicosis-water deprivation was considered to be an unlikely cause of the condition. In addition, water availability was not problematic on any of the affected farms.
Polioencephalomalacia is best documented in ruminants. In cattle, PEM is the result of thiamine deficiency (due to thiaminase-producing bacteria or plants or to true dietary deficiency), sulfur intoxication, lead poisoning, or water deprivation.14 In ruminants, PEM is characterized by laminar cortical necrosis, with necrotic areas grossly exhibiting yellow-green autofluorescence under 365-nm ultraviolet light. This characteristic was historically attributed to the accumulation of ceroid-lipofuscin in lipophages subsequent to lipid degeneration in injured neuronal cell membranes. However, more recently, it was proposed that intracytoplasmic subunit c of mitochondrial ATP synthetase may be responsible for the autofluorescence.14 Some cases also exhibit focal symmetric necrosis in the thalamus, colliculi, or brainstem; however, this is more typical of thiamine deficiency in carnivores.15 Most of the pigs examined at NCSU in this series exhibited both laminar cortical necrosis and degenerative changes in the periventricular grey matter.
The proposed mechanism for sulfur toxicosis in ruminants involves metabolism of ingested sulfur compounds to hydrogen sulfide gas by ruminal microbes. This toxic gas is either absorbed though the ruminal wall or eructated and inhaled. Hydrogen sulfide is thought to inhibit cytochrome oxidase and interfere with aerobic metabolism in the brain. However, it also may be involved in the formation of free radicals or act as an exogenous neuromodulator.16 It was unfortunate that sulfur content in the diet or drinking water was not evaluated in the present case. Attempts to induce neuronal lesions in 10-week-old, 7- to 14-kg pigs through thiamine-deficient diets historically have been unsuccessful.7 Experimentally induced thiamine-deficiency in pigs caused cardiac dilation and hypertrophy with myocardial necrosis.7 These histological lesions were not routinely evident in the pigs showing clinical signs and submitted to the various diagnostic laboratories.
On the basis of the positive response to supplemental thiamine injections, it was suspected that the thiamine in the diet was either destroyed or unavailable. Thus, additional thiamine was added to the vitamin premix. Animals do not synthesize thiamine and obtain daily requirements from their diets, storing excesses in the liver. Metabolic disorders are associated with thiamine deficiency; among the attendant clinical signs are diarrhea, reduced growth rate, weight loss, and anorexia, while central nervous system disorders usually manifest with severe depletion at a later stage of thiamine deficiency. It is speculated that the apoenzyme-thiamine complexes in the brain, which protect the brain tissue from sudden changes in enzyme activity, are responsible for this clinical presentation. Body reserves are reported to be sufficient for only 3 weeks in ruminants, but are not documented for swine.17 Even though thiamine is active in most cells, cells of the nervous system and heart seem particularly sensitive to the effects of thiamine deficiency.18
The clinical presentation of thiamine deficiency in humans is similar to the clinical signs noted in the present case. Thiamine deficiency is not uncommon in human populations in the Far East, where infants suckling from thiamine-deficient mothers develop clinical signs of beriberi syndrome and slow growth rates.19 Beriberi refers to the lack of thiamine pyrophosphate, which is the active form of thiamine in humans. Thiamine stores are usually depleted within 1 month, and clinical signs, beginning as early as 1 week after the last ingestion, include weakness and peripheral neuropathy. The “dry” form of beriberi refers to the neurologic disease where individuals have impairment of sensory, motor, and reflex functions of the extremities due to degeneration of myelin in the muscular sheaths.20
The “wet” form of beriberi refers to a thiamine deficiency with cardiovascular involvement, where peripheral vasodilation occurs, causing high cardiac output. This initiates water and sodium retention through the renin-angiotensin-aldosterone system, which ultimately results in fluid overload, peripheral edema, and myocardial injury. If this occurs acutely, there can be fatal fulminant cardiac failure.20 This cardiovascular involvement possibly contributed to the pathogenesis of severe pulmonary edema and sudden death observed in the older population of pigs in the present case.
With the presentation of periweaning-age pigs being affected, it was likely that inadequate thiamine was transferred through the milk. In one study,19 rats were fed a thiamine-deficient diet during the latter stages of gestation and the entire lactation phase. When the dams were fed the thiamine-deficient diet, transfer of thiamine from the dam to the pups was reduced after day 12 of lactation. Extrapolating to the present case, the sows’ stores of thiamine became depleted as lactation progressed, and the piglets no longer received adequate thiamine in the milk. Presumably, the sows were not affected because reserves of thiamine were greater. An early study successfully induced thiamine deficiency in young pigs.21 Pigs were taken from sows at 3 or 4 days of age and fed a thiamine-depleted diet. Pigs appeared clinically normal for the initial 12 days, but became weak, started vomiting, and died within 4 weeks. Heart lesions were noted in thiamine-deficient pigs, but not in pigs that were necropsied after supplementation of thiamine.21 These observations confirm the time frame of clinical disease observed in the periweaning pig population in the present case; however, myocardial lesions were not observed in this case. Rather, the neurological lesions were consistent with the clinical signs.
The authors do not recommend routine supplementation of diets with thiamine, nor do we believe that thiamine injections are required under normal circumstances on commercial farms. In the present case, compromised dietary thiamine levels during feed manufacturing contributed to the PEM.
Implications
• Pigs may develop histological lesions similar to those reported in ruminants affected with PEM.
• In this case, the causation diagnosis of thiamine destruction in the feed is speculative; however, practitioners need to consider thiamine deficiency as a potential cause of neurological disorders in young pigs.
Conflict of interest
None reported.
Disclaimer
Scientific manuscripts published in the Journal of Swine Health and Production are peer reviewed. However, information on medications, feed, and management techniques may be specific to the research or commercial situation presented in the manuscript. It is the responsibility of the reader to use information responsibly and in accordance with the rules and regulations governing research or the practice of veterinary medicine in their country or region.
References
1. Cebra C, Loneragan G, Gould D. Polioencephalomalacia (cerebrocortical necrosis). In: Smith BP, ed. Large Animal Internal Medicine. 4th ed. St Louis, Missouri: Mosby Elsevier. 2009:1022–1026.
2. Reese DE, Hill GM. Trace minerals and vitamins for swine diets. In: Meisinger DJ, ed. National Swine Nutrition Guide. Ames, Iowa: Iowa State University. US Pork Center of Excellence. 2010:41–52.
3. Reese DE, Miller PS. Nutrient deficiencies and excesses. In: Zimmerman JJ, Karriker LA, Ramirez A, Schwartz KJ, Stevenson GW, eds. Diseases of Swine. 10th ed. Ames, Iowa: Wiley-Blackwell. 2010:923–937.
4. National Research Council. Vitamins. In: Nutrient Requirements of Swine. 11th rev ed. Washington, DC: The National Academies Press; 2012;114–115.
5. Ellis NR, Madsen LL. The thiamine requirement of pigs as related to the fat content of the diet. J Nutr. 1944;27:253–262.
6. Gibson DM, Kennelly JJ, Aherne FX. The performance and thiamin status of pigs fed sulfur dioxide treated high-moisture barley. Can J Anim Sci. 1987;67:841–854.
7. Follis RH, Miller MH, Wintrobe MM, Stein HJ. Development of myocardial necrosis and absence of nerve degeneration in thiamine deficiency in pigs. Am J Path. 1943;19:341–357.
8. Newman AJ. Suspected thiamine deficiency in pigs. Vet Rec. 1969;84:577–578.
9. Okada HM, Chihaya Y, Matsukawa K. Thiamine deficiency encephalopathy in foxes and mink. Vet Path. 1987;20:180–182.
10. Read DH, Jolly RD, Alley MR. Polioencephalomalacia of dogs with thiamine deficiency. Vet Path. 1977;14:103–112.
11. Studdert VP, Labuc RH. Thiamine deficiency in cats and dogs associated with feeding meat preserved with sulphur dioxide. Aust Vet J. 1991;68:54–57.
12. Jubb KV, Saunders LZ, Coats HV. Thiamine deficiency encephalopathy in cats. J Comp Path. 1956;66:217–227.
13. Milad KE. The occurrence of thiamine-responsive polioencephalomalacia in dromedary breeding camels in Libya: preliminary investigation of diagnosis. Iraqi J Vet Sci. 2009;23(Suppl I):119–122.
14. Rachid MA, Rilho EF, Carvalho AU, Vasconcelos AC, Ferriera PM. Poliocephalomalacia in cattle. Asian J Anim Vet Adv. 2011;6:126–131.
15. Zachary JF, McGavin MD. Pathologic Basis of Veterinary Disease.5th ed. St Louis, Missouri: Elsevier Mosby. 2012:849–852.
16. Haydock D. Sulfur-induced polioencephalomalacia in a herd of rotationally grazed beef cattle. Can Vet J. 2003;44:828–829.
17. Rammell CG, Hill JH. A review of thiamine deficiency and its diagnosis, especially in ruminants. New Zealand Vet J. 1986;34:202–204.
18. Martin PR, Singleton CK, Hiller-Sturmhöfel S. The Role of Thiamine Deficiency in Alcoholic Brain Disease. National Institute on Alcohol Abuse and Alcoholism, National Institutes of Health, United States Department of Health and Human Services; Bethesda, Maryland; 2004.
19. Trostler N, Sklan D. Milk composition and thiamine transfer in thiamine deficient rats. Am J Clin Nutr. 1977;30:681–685.
20. Dieu-Thu NK. Beriberi (thiamine deficiency). Emedicine, Medscape. 2011. Available at: http://emedicine.medscape.com/article/116930-overview. Accessed 14 February 2015.
21. Miller ER, Schmidt DA, Hoefer JA, Luecke RW. The thiamine requirement of the baby pig. J Nutr. 1955;56:423–430.